


























COVID-19: Myths vs. facts
Here’s what you need to know about novel Coronavirus
Image from U.S. National Park Service
The hot topic of the year: coronavirus. While everybody knows the basics, there’s a lot of misinformation going around. That’s why we’ve assembled a fast facts story about the myths of the novel coronavirus and the facts that contradict them.
While it’s true that COVID-19 and the flu share many qualities, the novel coronavirus is a very different situation from the flu, and should be treated as such. We have decades upon decades of experience dealing with the flu, and a few scant months of experience dealing with COVID-19.
The coronavirus is about twice as contagious, has no vaccine, and has an average death-per-case rate roughly 12 to 24 times higher than that of the flu based on data from the China outbreak, according to the World Health Organization (WHO).
One of the most common misconceptions with the coronavirus is that the danger comes from the likelihood of the average person dying, which is very low. This assumption makes people think increasing hygiene, closing down schools, et cetera, is way overboard. It’s not.
The danger of coronavirus comes from the likelihood that our hospitals will be overwhelmed, which is very high. According to NPR, Italian hospitals are scrambling to find enough beds and medical professionals are forced to choose who gets to use life-saving medical equipment.
According to CBS, the best case scenario is for 20% of the US’ adult population to be infected over the course of 18 months, which would result in hospitals being strained but still functional at 95% capacity. Lower that time period to six or even twelve months, and hospitals are completely overwhelmed.
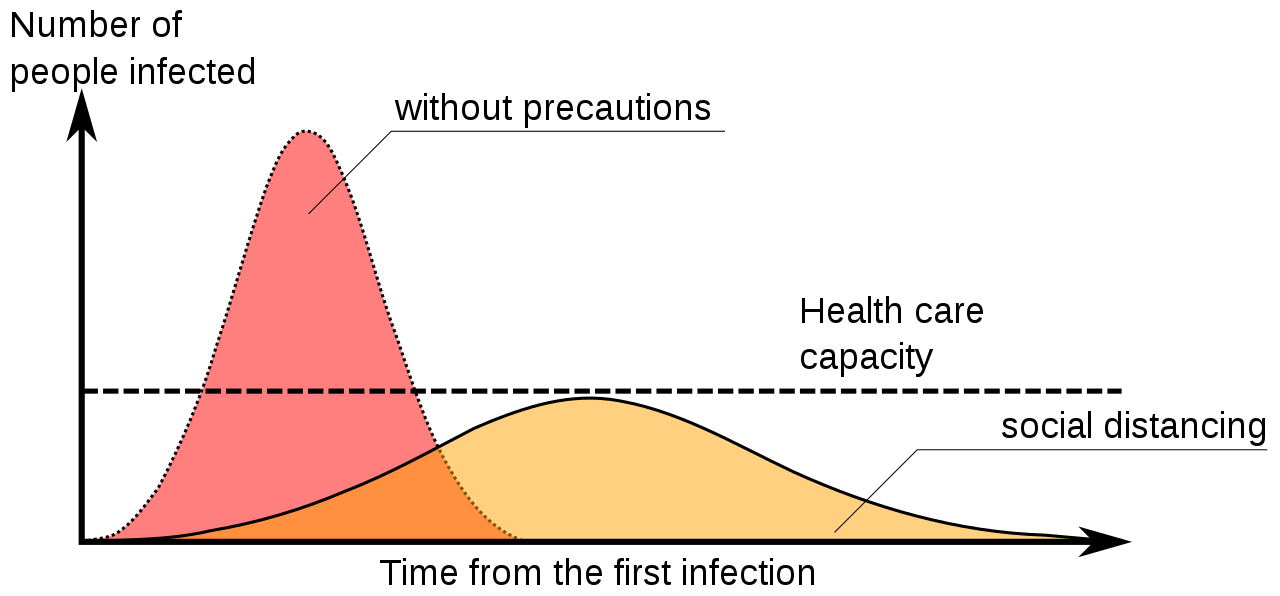
In order to relieve the stress on hospitals, we must “flatten the curve.” No doubt you’ve heard this, but what is flattening the curve, exactly? Flattening the curve refers to reducing the number of cases and slowing the spread of COVID-19 so that hospitals can handle the influx. On the graph below, the blue curve represents case numbers after measures taken to, quite literally, flatten it.
The US is already well beyond the point that Wuhan was at when it completely shut down. Assuming everything will be fine and life can go on as normal will only put the elderly those with compromised immune systems at risk, and many low-wage workers in jobs such as fast food cannot afford to take time off work or get treated, possibly infecting hundreds of people. The United States is not immune to strife and disease, no matter how safe and affluent we seem.
In addition to this, testing in the US is largely incomplete, and much of the data we have is possibly hundreds to even thousands below the actual number of US cases. This is making it seem like the situation is much less dire than it actually is, and leading a lot of people to assume shrugging off precautionary measures like social isolation is okay.
However, this does not mean we should be panicking and stocking up on supplies such as masks and hand sanitizer. Our hospitals are already running low on masks, and while surgical masks are relatively harmless to buy, high-quality N95 masks are completely essential to our healthcare system. There is no extra store of masks for hospitals, and we as the people must be careful to not monopolize resources desperately needed by those on the front lines of the crisis.
In addition, there’s been a lot of misinformation spreading around when and how the coronavirus can be transmitted. In contrast to the assumption that COVID-19 cannot be transmitted in warm weather and mosquitoes are capable of transmitting the novel coronavirus, the WHO reports that the novel coronavirus can be transmitted in any weather, and not by mosquitoes.

Lia Farrell is an editor for the Pack and the proud founder of #petsofmonarch on the mohimix Instagram. If she isn’t in the Hub or doing work for her...